The COVID-19 epidemic may rebound around the Spring Festival! We sorted out the information about the new strain
At a recent press conference of the State Council Information Office, the relevant person in charge of the National Administration of Disease Control and Prevention stated that due to the sharp increase in the flow of people during the Spring Festival, it is expected that the new crown epidemic may rebound to a certain extent around the Spring Festival, and many parts of the country will continue to experience a variety of respiratory diseases. Or common epidemic situation.
So, how toxic is the new coronavirus strain JN.1? Can influenza and COVID-19 be cross-infected?
So, how harmful is the latest JN.1?
Judging from global data, the new coronavirus JN.1 spreads quickly, but the risk has not increased.
JN.1 is the second-generation sub-branch of the Omicron BA.2.86 variant, which was first monitored in Luxembourg at the end of August last year.
According to the latest data from GISAID, JN.1 began to spread around the world in November last year. In just one month, it became the mainstream strain globally, accounting for 50% of daily new cases. Currently, this proportion has exceeded 70% and has spread to at least 59 countries and regions around the world.
Faster transmissibility is also reflected in wastewater viral activity levels. The higher the value of this indicator, the more widespread the virus is.
According to data from the U.S. Centers for Disease Control and Prevention, during the week of December 30, the concentration level of the new coronavirus in wastewater across the United States was 12.85, reaching the second highest peak in history since the outbreak of the new coronavirus in the United States.
Relevant scholars said that compared with the previous new coronavirus, the JN.1 virus has acquired a key new mutation, so its ability to spread is stronger.
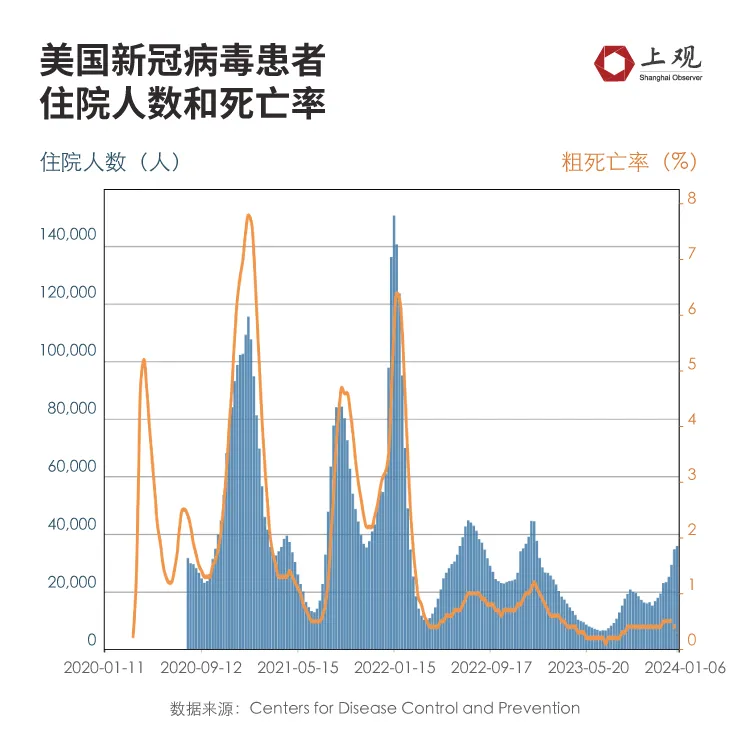
Judging from the hospitalization situation and case fatality rate, the influence of JN.1 has not exceeded that of previous strains.
According to data from the US CDC, during the week of January 6, the number of new hospitalization applications due to COVID-19 infection was 35,800, an average of about 11 people per 100,000 people.
Although the trend has increased, it is not too serious compared with the previous peak. At the beginning of 2022, the peak number of people applying for hospitalization due to COVID-19 infection in the United States was approximately 45.5 per 100,000 people, which is 4.4 times the current rate.
Judging from the death toll situation, the number of deaths from COVID-19 in the United States is declining.
In the week of January 6, the number of deaths due to the new coronavirus was 0.3 per 100,000 people. Last year's peak was 1.2 per 100,000 people, which was also about 4 times the current level.
If compared with 2020, the gap is even greater, about 26 times the current level.
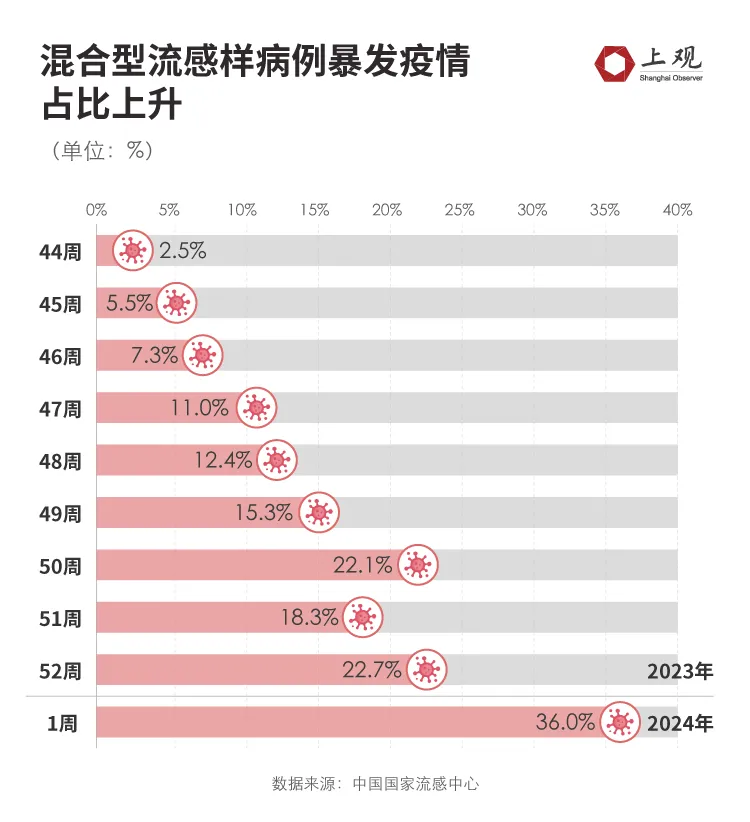
At present, the positive rate of influenza virus testing in China has dropped somewhat, but among them, firstly, the proportion of influenza B is increasing, and secondly, the proportion of mixed infections has increased recently. It may manifest itself as being infected at the same time, or it may be the case of "influenza A just happened to be infected with influenza B".
According to data from China's National Influenza Center, the proportion of mixed infections increased to 36% in the first week of 2024, compared with only 12.4% a month ago.
With the spread of JN.1, will people who have had the flu still be infected with the new coronavirus?
Judging from research data, it is possible, but the proportion is not high.
According to a paper published two years ago by scholars at France's Aix-Marseille University [1], it included and analyzed 54 relevant studies from around the world, including data on approximately 18,000 new coronavirus-infected patients.
The results showed that the proportion of co-infections with COVID-19 and influenza was only 0.7%, which means that among 18,000 patients, only about 140 patients were infected with the COVID-19 virus and influenza virus at the same time.
However, compared with influenza B, influenza A is more likely to be co-infected with COVID-19.
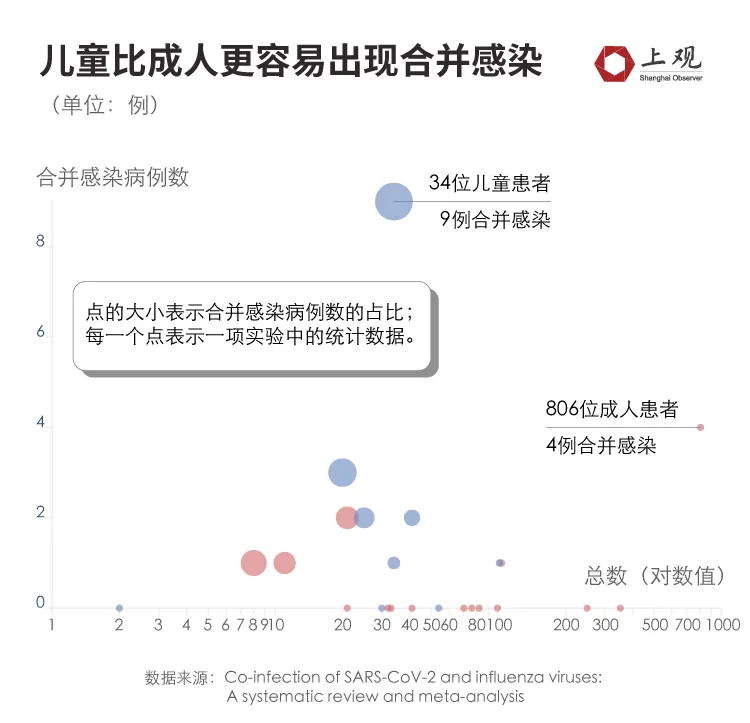
Data show that among the 143 co-infected patients, 74% were infected with influenza A and 20% were infected with influenza B. Only one patient was infected with three viruses at the same time, which is a low probability. Breaking down the age of the patient, children are more likely to have co-infections than adults.
Data show that the proportion of children with co-infections is 3.2%, which is about 10 times the proportion of adult patients.
Although the possibility of co-infection is very low, once infected, the condition may be aggravated.
As early as 2021, the National Key Experiment in Virology found that in the experimental mice, co-infection would cause more cells and tissues in the body to be attacked by the virus, which would then cause more severe pathological reactions in the lungs, with a large number of cell infiltrates and obvious Alveolar necrosis [2].
From the comparison of patient data, co-infection will indeed lead to more severe symptoms of patients.
According to a paper published by Nanjing Medical University in 2022 [3], compared with patients who are single-infected with the new coronavirus, patients with co-infections are more likely to need to use a ventilator, and the risk is 2.31 times higher than that of single-infected patients.
Among them, the risk of using a ventilator when infected with COVID-19 and influenza A at the same time is higher, 5.04 times that of a single infection.
Symptoms mainly focus on respiratory complications, such as acute hypoxic respiratory failure, acute respiratory distress syndrome, cardiac injury, and acute kidney injury.
Not only that, patients with co-infections are also more likely to be admitted to the ICU.
Research shows [3] that the risk of co-infected patients being admitted to the ICU is 2.09 times that of patients with a single infection.
According to a paper published in the "International Journal of Epidemiology" in 2021 [4], in the face of co-infection, the elderly group has a greater probability of severe illness and is more likely to be life-threatening.
For example, among patients aged 50-59, 60% were admitted to the ICU after co-infection, while 24% had a single infection. Among patients aged 80 and above, the proportion of deaths after coinfection was 66.7%, which was also higher than the proportion of single infection.
However, coinfections may not increase the risk of death. Studies have shown [3] that there is a significant association between co-infection status and death.
Including the elderly, young children and high-risk groups with underlying diseases, they need to pay attention to timely differential diagnosis when upper respiratory tract infection symptoms appear and take relevant drugs to relieve symptoms, shorten the course of the disease, and reduce the risk of severe illness and hospitalization.
【1】Dao,TL,Colson,P.,Million,M.,&Gautret,P..Co-infectionofSARS-CoV-2andinfluenzaviruses:asystematicreviewandmeta-analysis.JournalofClinicalVirologyPlus,1,100036.
【2】Bai,L.,Zhao,Y.,Dong,J.,Liang,S.,Guo,M.,Liu,X.,...&Xu,K..CoinfectionwithinfluenzaAvirusenhancesSARS-CoV-2infectivity.Cellresearch,31,395 -403.
【3】Cong, B., Deng, S., Wang,
【4】Stowe,J.,Tessier,E.,Zhao,H.,Guy,R.,Muller-Pebody,B.,Zambon,M.,...&LopezBernal,J..Interactions between SARS-CoV-2andinfluenza,andtheimpactofcoinfectionondiseaseseverity :test-negativedesign.InternationalJournalofEpidemiology,50,1124-1133.