How to no longer "sink"?, 10000 fewer village clinics in a year: medical resources "sinking" rural services | grassroots | medical care
Introduction: The scarce amount of diagnosis and treatment not only causes the newly added medical resources in these township health centers and village clinics to be idle and wasted, but also frequently puts them in operational difficulties.
Since the top-level design of the medical consortium construction was released in 2017, the "County Medical Community" has entered its sixth year. This institutional arrangement, which has been closely related to the construction of a hierarchical diagnosis and treatment orderly medical treatment pattern since its inception, has shown initial effectiveness in promoting the return of medical services to counties. But compared to "strong counties", "strong grassroots" faces more severe challenges.
For a long time, the unreasonable allocation and utilization of health resources have led to a lack of trust in rural grassroots medical and health service capabilities among township patients. In addition, the benefit sharing mechanism for promoting the hierarchical diagnosis and treatment system within the county medical community still needs to be improved. A large number of patients flow to county hospitals, and even public comprehensive hospitals in big cities, resulting in a continuous decline in the volume of rural grassroots diagnosis and treatment. The scarce amount of diagnosis and treatment not only causes the newly added medical resources in these township health centers and village clinics to be idle and wasted, but also frequently puts them in operational difficulties.
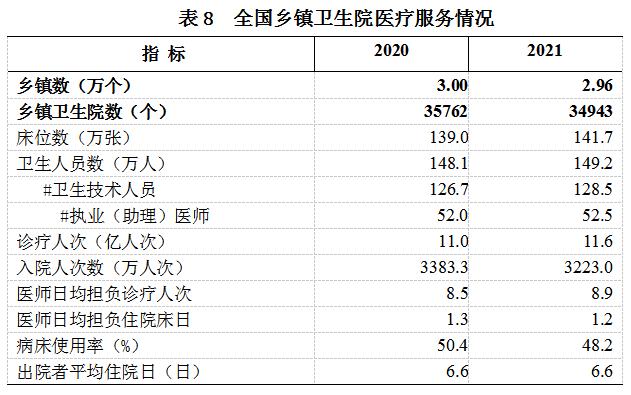
The latest statistical yearbook shows that in 2021, the average annual diagnosis and treatment volume in each village clinic was only 2239 people, which is equivalent to only 6 patients seeking medical treatment every day. In the same year, the number of township health centers and village health clinics decreased by 819 and 10000 respectively compared to the previous year.
Since the beginning of this year, the rational allocation of medical and health resources at the rural and county levels in county-level medical communities has been placed in a more prominent position. As of early June, multiple provinces including Fujian, Zhejiang, Shandong, Henan, Guangdong, and Sichuan have held the 2023 Provincial Grassroots Health Work Conference, with a focus on "optimizing and improving the basic medical and public health service capabilities at the grassroots level".
With the changes in the demand and structure of county-level medical services and the improvement of the supply level of basic medical services, how can township health centers and village clinics play a greater role in county-level medical communities? What bottlenecks still need to be overcome? First Financial recently interviewed Liu Yuanli, a counselor of the State Council and Executive Dean of the School of Health Management Policy at Peking Union Medical College.

Be wary of high-quality resources sinking into sinking
In February of this year, the General Office of the Communist Party of China Central Committee and the General Office of the State Council issued the "Opinions on Further Deepening Reform and Promoting the Healthy Development of Rural Medical and Health Systems.". It is mentioned that according to the changes in rural morphology and population migration and flow, rural medical and health resources at both levels should be reasonably allocated according to local conditions. For example, when it is suitable for the township, it is suitable for the township, and when it is suitable for the village, it is necessary to improve the individual scale and service radiation capacity of rural medical and health institutions, shifting from focusing on full coverage of institutions to paying more attention to full coverage of services.
What are the practical reasons for the proposal of shifting from focusing on full institutional coverage to paying more attention to full service coverage? Does it mean that the measurement scale of accessibility and fairness of basic medical services in rural areas has been adjusted?
Liu Yuanli: The so-called "shift from emphasizing full coverage of institutions to paying more attention to full coverage of services" is to complete the change in the concept and strategy of medical and health resource allocation, break administrative divisions, make overall planning more targeted, and allocate resources based on actual needs to achieve efficiency improvement.
The core of "emphasizing full service coverage" lies in matching. On the one hand, China has a vast territory and there are significant differences in environmental factors in different regions. Simply pursuing full institutional coverage may only achieve formal averaging.
For example, in the same western region, the population of a township in Sichuan may be equal to the population of a region in Xizang. If the construction is carried out according to the established establishment of "every village should have a health office, and every township should have a health center", then in the context of "county medical and health integration", it is necessary to equip these grass-roots institutions with corresponding high-end talents and equipment. On the surface, high-quality resources have sunk, but in fact, "sinking" has become "sinking", which does not actually play a role.

On the other hand, it is an undeniable fact that the total number of rural doctors has decreased in recent years. At the same time, whether local financial resources can support construction, maintenance and operation, provide subsidies for personnel, and conduct regular assessments is also a question mark.
If the same financial investment is used to provide business training for village doctors, increase their treatment level, and equip more portable diagnostic and treatment equipment for rural grassroots medical institutions, both disease prevention and control capabilities and the sense of medical access of villagers will be more significantly enhanced in the short term. In the long run, the marginal effect and sustainability of the investment will also be higher.
In addition, the Opinion emphasizes "full service coverage", which can be understood in reverse as the current supply of medical and health services at the rural level has not yet covered all needs.
In recent years, with the improvement of farmers' income level, health awareness and urban and rural transportation infrastructure, the rapid growth of incidence rate and coexistence of common diseases, frequently occurring diseases, chronic diseases and other basic diseases, the total amount of medical demand, demand levels and demand structure of rural residents are undergoing a leap, which is far faster than the increase speed of rural medical supply side. The contradiction between supply and demand of rural medical resource allocation is more prominent. The latter may also aggravate the siphon effect of county hospitals and urban hospitals.
From this perspective, achieving full coverage of rural grassroots medical and health services requires adapting to local conditions, adjusting the content of the original "grassroots service package" in a timely manner according to the changing trends of local rural disease spectrum, payment capacity and willingness.
The "service package" for rural primary healthcare is still not sound
First Finance: Currently, in county-level medical communities, what are the contents of the "service packages" of grassroots medical and health service institutions? What adjustments do grassroots service packages need to make in response to the complex and diversified trend of the aforementioned needs? What factors will constrain it?
Liu Yuanli: According to the top-level plan of "Healthy China", prevention is the main focus, with grassroots as the key, protecting key populations, and preventing and controlling major diseases. In this context, the "service package" of rural grassroots medical and health institutions should simultaneously meet the goal requirements of "three comprehensive".
For township health centers and village clinics, "full process" means exploring the implementation of a single disease group management path, treating patients with the same disease as a group, optimizing and integrating secondary prevention, tertiary prevention, clinical medical treatment, and disease rehabilitation, and establishing a health management model with six links of "promoting prevention, diagnosis, control, and treatment".
Due to the different foundations of rural grassroots medical and health services in different regions, there are also differences in the main health problems and risk factors of the population within the region. Therefore, the "full coverage" of rural grassroots medical and health resources is not comprehensive, but rather filling in the gaps. Similarly, whether and how to expand the "grassroots service package" should be tailored to local conditions to address the weaknesses and strengths in promoting prevention, diagnosis, control, and treatment.
The current prominent problem is the lack of integration between medical and preventive measures, which is the disconnect between prevention and treatment.
On the one hand, this is related to the inadequate "service packages" at the grassroots level in rural areas. In many rural areas, there is already a certain foundation in the treatment of basic diseases, but the public awareness rate of diseases is low. Grassroots medical personnel focus more on the prevention of infectious diseases, and do not pay enough attention to chronic non communicable diseases, mental illnesses, and other related issues.

On the other hand, under the existing administrative and management framework, there is insufficient coordination between local disease control departments and grassroots medical and health institutions, resulting in the difficulty of fully realizing the "prevention" function in grassroots service packages.
Rehabilitation is another easily overlooked issue. In the county-level medical community, for diseases that need to be transferred to higher-level hospitals for treatment, many patients still need post-treatment rehabilitation, and this service can be transferred to grassroots medical care. But if the "grassroots service package" does not cover it, it will squeeze out the resources of county hospitals and increase the treatment costs for patients in higher-level hospitals. Of course, a more common and serious problem is that due to the lack of emphasis on timely rehabilitation services by medical insurance providers, healthcare providers, and patients, patients often lose the golden window of rehabilitation intervention.
"Full cycle" means that rural grassroots medical and health institutions need to provide a series of medical services from birth to death, from maternal health care to end-of-life care. Among them, a portion of medical and health services are included in the basic public health services targeting high-risk groups such as children, pregnant and postpartum women, the elderly, and patients with chronic diseases.
Although basic medical and health services in rural areas have public welfare attributes, there are significant differences in the guarantee mechanisms between basic medical services and basic public health services, which restricts the actual implementation of "full cycle" medical and health services at the grassroots level. Specifically, basic public health services are provided free of charge to key populations with government financial support, while basic medical services require patients to self pay or obtain medical insurance.
Whether the "service package" of rural grassroots medical and health institutions can be expanded depends on the coordination and integration between medical and disease control departments, county-level medical institutions, medical, pharmaceutical, and medical insurance policies, as well as local finance at multiple levels such as medical and health expenditure and total economic and social development expenditure. To promote fairness and equality in rural basic medical and health services between regions and populations, it is necessary to promote fair coverage through fair financing.
Promoting the construction of a close medical community through organized fundraising
First Finance: There is a significant gap in economic foundations among different regions. How can you achieve the "fairness in fundraising" you mentioned?
Liu Yuanli: Firstly, the central government has always supported rural medical and health institutions through subsidies for basic public health services and basic drug systems, and provided subsidies to improve the capacity of rural grassroots medical services in difficult areas in accordance with regulations.
The Opinion also clearly states that the central budget should increase investment in leading medical institutions in the county-level medical service system, with a focus on supporting the construction of county-level hospitals in poverty-stricken areas, former central Soviet areas, and relocated areas for poverty alleviation. Local governments are shifting their financial resources towards rural healthcare.
Secondly, increase the collaborative support of medical insurance policies for grassroots medical and health services. For example, under the national basic drug system, the quantity and quality of drug supply at the grassroots level in rural areas are directly and indirectly affected by medical insurance. Therefore, medical insurance plays a "leading role" in healthcare and medicine.
Thirdly, to achieve organized fundraising, that is, to promote the integration ability of multi-channel funds such as government financial investment, social medical insurance, and commercial health insurance. For example, basic medical insurance and medical assistance subsidy funds are managed by different departments, but may serve the same target. At the same time, it is necessary to improve the design and payment methods of welfare packages.
In the context of a county, achieving the integration of the medical and health security system at the county, township, and village levels is a prerequisite for achieving organized financing.
Taking medical insurance as an example, currently, some local medical insurance funds do not have enough support for grassroots medical services. Multiple basic diseases have not achieved equal distribution and price among medical institutions at all levels in the county, or the coverage of basic diseases that can be reimbursed in grassroots medical and health institutions is limited and updated slowly. This leads to disease diagnosis and treatment services that can be triaged at the grassroots level flowing into higher-level medical institutions.
Therefore, it is necessary to reasonably increase the total control index of the medical insurance fund for rural medical and health institutions. The focus of the annual new medical insurance fund is to tilt towards rural medical and health institutions, and gradually increase the proportion of medical insurance funds used for rural medical and health services within the county. The effective implementation of "strengthening grassroots" can promote the quality and efficiency of the entire medical and health system.




